Child Not Eating Rice, Force-Feeding Makes It Worse — Causes, Management, and Diagnostic Criteria for Poor Appetite

 🧾 Answer First | Core Conclusion
🧾 Answer First | Core Conclusion
When a child takes just a few spoonfuls of rice and stops, parents carry heavy hearts all day long.
I am Dr. Choi Jang-hyuk, a Korean medicine practitioner and director of Dongjedang Korean Medicine Clinic.
Poor appetite in children is mostly a normal change during periods when growth slows down, and force-feeding only intensifies refusal.
After age one, as growth slows down, the amount eaten naturally decreases, and a period of rejecting new foods follows.
There are three things to check now:
Returning the decision-making power over eating amounts to the child,
Reducing snacks and beverages before meals,
And judging by growth curve trends rather than the amount per meal.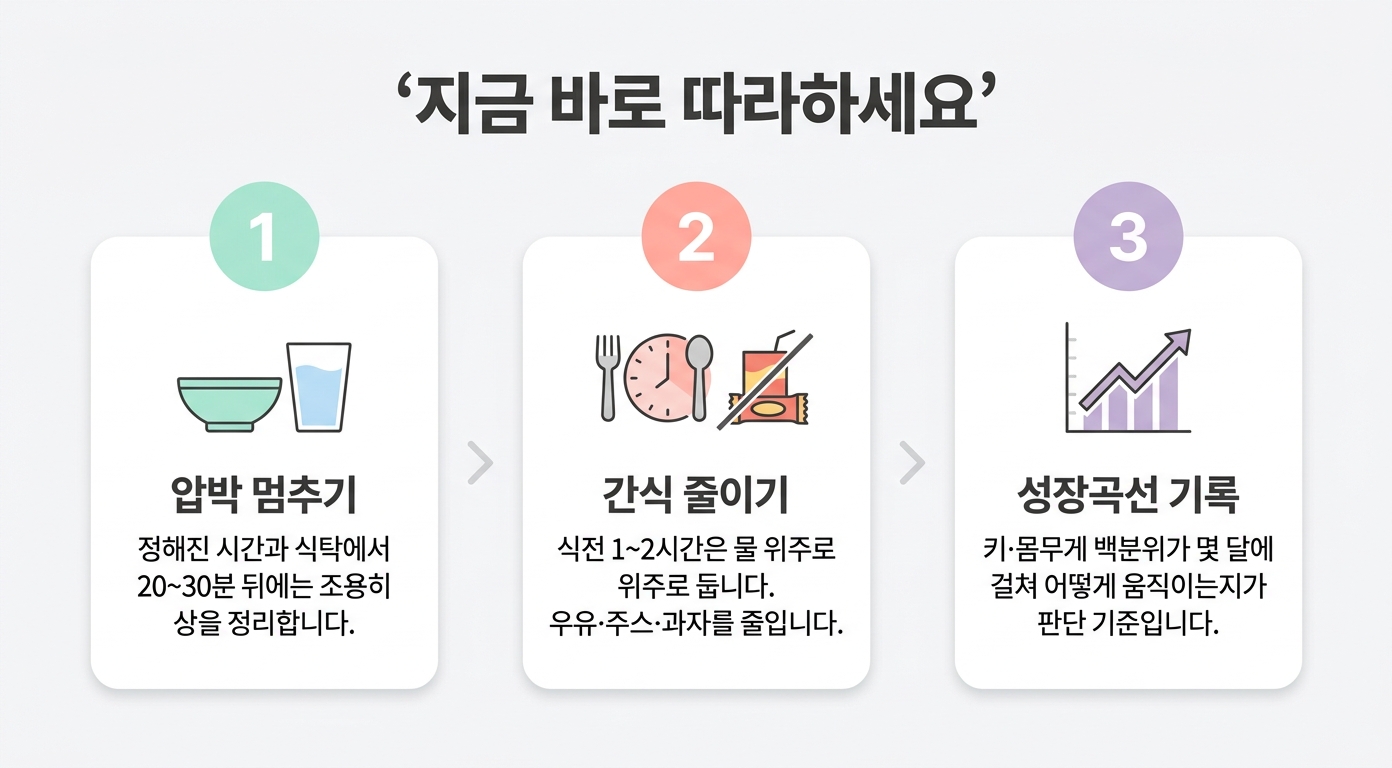 ✅ Action | Immediate Implementation — What should you do when a child won't eat rice?The key is for parents to decide what, when, and where to feed, while letting the child decide how much to eat.
✅ Action | Immediate Implementation — What should you do when a child won't eat rice?The key is for parents to decide what, when, and where to feed, while letting the child decide how much to eat.
1️⃣ Stop pressure to eat. Discontinue "one more bite," chasing the child to eat, and scolding.
After 20-30 minutes at the set mealtime and table, quietly clear away the dishes.
2️⃣ Reduce snacks and beverages 1-2 hours before meals.
Many children become full from milk, juice, or snacks, or skip meals due to juice calories. During that time, offer mainly water.
3️⃣ Record the growth curve.
The standard for judgment is not the amount per meal, but how height and weight percentiles move over several months.
After a few weeks of this approach, most children naturally regulate their own intake. However, if the following signals appear, things are different.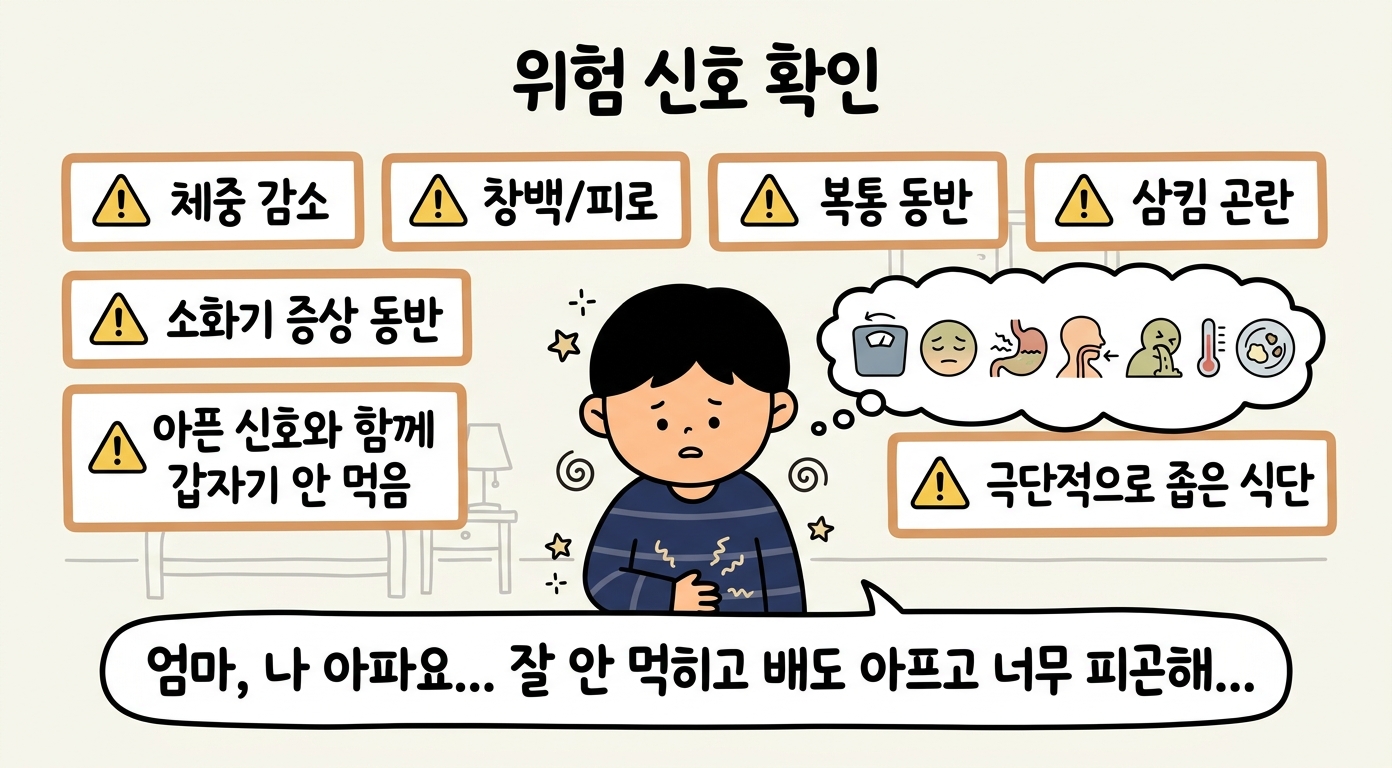 🚨 Warning | Warning Signs That Must Be Checked — When should you go to the hospital?If weight decreases or the growth curve bends downward with paleness, fatigue, and abdominal pain, medical consultation is necessary.
🚨 Warning | Warning Signs That Must Be Checked — When should you go to the hospital?If weight decreases or the growth curve bends downward with paleness, fatigue, and abdominal pain, medical consultation is necessary.
✔ Weight loss or plateau Weight decreases or the growth curve crosses below the percentile.
✔ Paleness and easy fatigue The face is pale and tires easily (suspected anemia).
✔ Difficulty swallowing There is choking, nausea, or pain when swallowing.
✔ Accompanying digestive symptoms Abdominal pain, constipation, or vomiting occur together.
✔ Sudden loss of appetite with illness signs Appetite suddenly drops along with signs of illness such as fever.
✔ Extremely limited diet The types of food eaten are very restricted and signs of nutritional deficiency appear.
If any one persists, it is best to first check for growth, anemia, and digestive problems.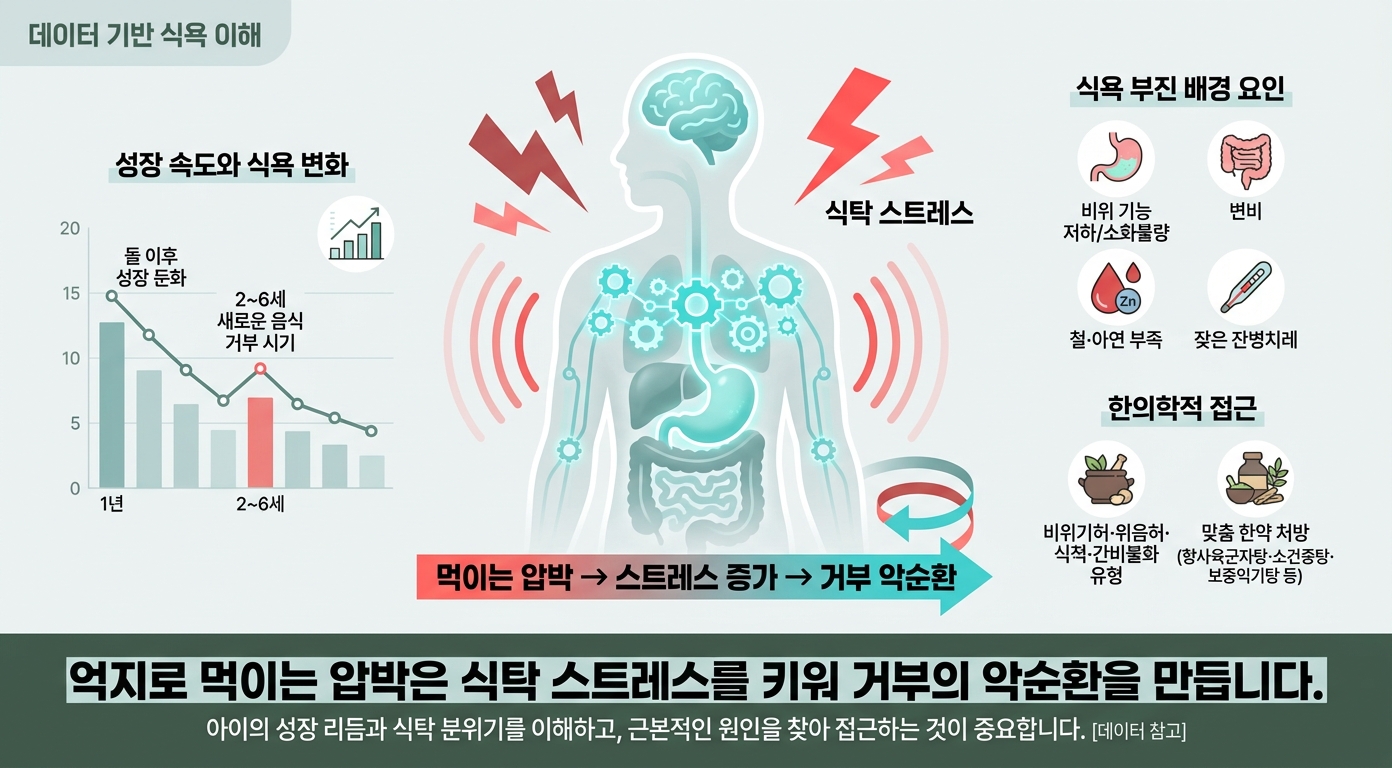 🧠 The Why | Cause Analysis — Why does force-feeding make it worse?A child's appetite is regulated according to growth rate, and pressure from force-feeding usually stems from worry about "eating too little," which ironically intensifies refusal.
🧠 The Why | Cause Analysis — Why does force-feeding make it worse?A child's appetite is regulated according to growth rate, and pressure from force-feeding usually stems from worry about "eating too little," which ironically intensifies refusal.
After age one, appetite naturally decreases as growth slows. Between ages 2-6, it is common for a period of rejecting new foods to coincide.
Pressure creates a vicious cycle. The more parents try to control feeding out of worry, the more the child learns to see mealtimes as stressful and refuses more.
In fact, controlling feeding methods are linked to picky eating, and it has been confirmed that as children eat less, parents apply more pressure [2].
It is neither because the child is stubborn nor because parents feed incorrectly. It is a phenomenon that emerges from the interplay of growth rhythm and mealtime atmosphere.
In some cases, weakened digestive function, indigestion, constipation, iron or zinc deficiency, or frequent minor illnesses are in the background.
In Korean medicine, such children are categorized into types like weakened spleen-stomach qi, stomach yin deficiency, food stagnation, and liver-spleen disharmony, and are treated with herbal medicines (Xiang Sha Liu Jun Zi Tang, Xiao Jian Zhong Tang, Bu Zhong Yi Qi Tang, etc.) tailored to the type [3]. This is why mealtimes become difficult the more anxious parents become when facing a child who takes just a few spoonfuls and stops.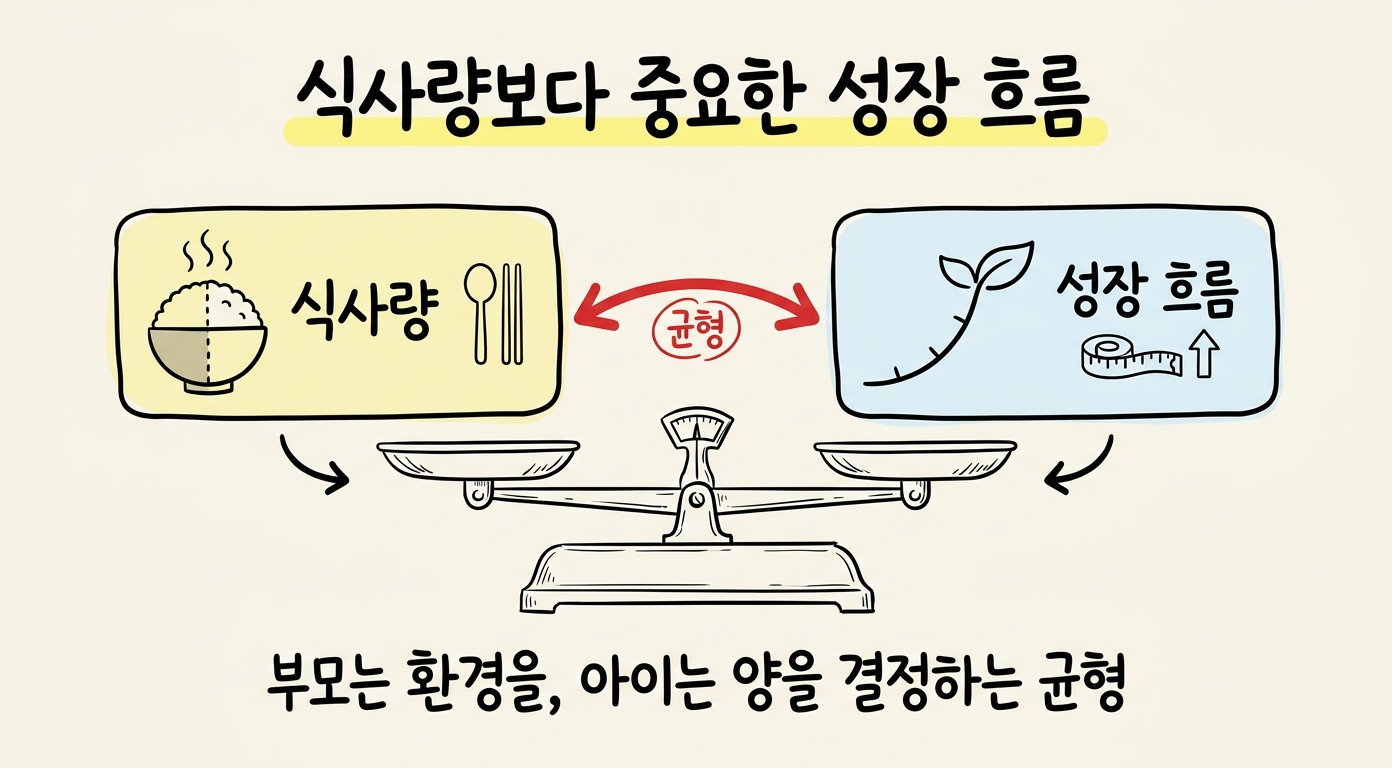 📊 Proof | Cases and Evidence — What should you first look at with a child who won't eat?Most poor appetite is an eating habit problem within the normal range, but when looking at digestive function and mealtime atmosphere together, the actual amount eaten actually differs.
📊 Proof | Cases and Evidence — What should you first look at with a child who won't eat?Most poor appetite is an eating habit problem within the normal range, but when looking at digestive function and mealtime atmosphere together, the actual amount eaten actually differs.
Pediatric poor appetite is one spectrum of feeding difficulties, presenting as rejection of even familiar foods or monotonous diet patterns [1].
A child came to me saying "no matter what I do, they won't eat." I first asked not how many grams they ate per day, but what kind of atmosphere mealtimes had. Every meal was a struggle. So I stopped the pressure to feed and took an approach to check the digestive state together.
That child didn't suddenly start eating well; their original rhythm returned once mealtimes became comfortable.
Evidence for Korean medicine treatment is also accumulating. The Korean Medicine Clinical Practice Guideline for Pediatric Anorexia recommends herbal medicine treatment (moderate evidence grade), and comprehensive clinical research results show that the herbal medicine group had increased weight and meal amount and reduced recurrence compared to placebo and standard treatment groups [4]. Mechanistic evidence is also reported that herbal medicine aids gastric emptying and raises appetite-related hormones (ghrelin and motilin) [4].
The prescriptions most commonly used by Korean medicine practitioners were Xiang Sha Liu Jun Zi Tang, Xiao Jian Zhong Tang, and Bu Zhong Yi Qi Tang [3]. However, since considerable portions of this evidence come from Chinese clinical research with limitations in blinding, pediatric evaluation is conducted together if there are growth reductions or warning signs.
What changed in that child was not the child themselves, but the tension surrounding eating loosened and the body's signals found their rightful place. 🔚 Closing | Summary and Encouragement
🔚 Closing | Summary and Encouragement
While you cannot forcefully boost a child's appetite, you can start now by returning the decision-making power over eating amounts and monitoring growth trends.
If symptoms do not improve even after stopping pressure and observing for a few weeks, or if there are warning signs, management that examines growth, digestive state, and spleen-stomach function together can help. At Dongjedang Korean Medicine Clinic's Pediatric and Test-Taking Student Clinic, we look at children's growth and digestive rhythms together.
✍️ Reviewed by Dr. Choi Jang-hyuk, Director of Dongjedang Korean Medicine Clinic · Dr. Choi Jang-hyuk, Director of Dongjedang Korean Medicine Clinic · Clinical specialist in pediatric and growth disorders | Review date: 2026-07-07
❓ FAQ
Q1. Should I force my child to eat if they won't eat rice? Force-feeding usually intensifies refusal. It is better in the long run if parents decide what, when to feed, and the child decides how much to eat.
Q2. Should I at least provide milk or snacks instead of rice? Milk, juice, and snacks 1-2 hours before meals actually cause children to skip meals. During that time, offer mainly water and have them eat at set mealtimes instead.
Q3. I'm worried that if they don't eat, they won't grow tall. The standard is the trend of height and weight percentiles rather than the amount per meal. If the growth curve is maintained, it is usually fine, and if it bends downward, confirmation is necessary. For more, see our article on height growth in children who neither eat rice nor sleep well.
Q4. Is Korean medicine treatment helpful? The Korean Medicine Clinical Practice Guideline for Pediatric Anorexia recommends herbal medicine treatment, and there are comprehensive clinical research results showing that the herbal medicine group had increased weight and meal amount with reduced recurrence compared to standard treatment [4]. However, since the certainty of evidence is moderate, pediatric evaluation should be conducted together if there are growth reductions or warning signs.
📚 References
The following medical evidence was confirmed from PubMed indexed articles and Korean Medicine Clinical Practice Guidelines.
[1] Taylor CM, et al. Picky/fussy eating in children. Appetite. 2015. (PubMed) — https://doi.org/10.1016/j.appet.2015.07.026
[2] Wang J, et al. Bidirectional Associations between Parental Feeding Practices and Child Eating Behaviors. Nutrients. 2023. (PubMed) — https://doi.org/10.3390/nu16010044
[3] Lee J, et al. Survey of Clinical Practice Patterns of Korean Medicine Doctors for Anorexia in Children. Children (Basel). 2022. (PubMed) — https://doi.org/10.3390/children9091409
[4] Korean Medicine Clinical Practice Guideline for Pediatric Anorexia. Evidence grade B (moderate). ※ [3] is a preliminary study for this guideline.
Pediatric
Child Not Eating Rice, Force-Feeding Makes It Worse — Causes, Management, and Diagnostic Criteria for Poor Appetite
View Program