Blog June 9, 2026
Connective Tissue Adaptive Response According to Stimulus Dose and an Integrated Model of Korean Medicine External and Internal Treatment — A Literature Review on the Action Coordinates of Acupuncture, Acupotomy, Heat-Assisted Moxibustion, Bee Venom Acupuncture, and Herbal Medicine

Jang-Hyuk Choi, KMD
Head Doctor
Table of Contents
- 1. Key Summary (Abstract)
- 2. Context of the Question (Introduction)
- 3. What the Literature Says (Results)
- 3-1. Connective Tissue Responds in Three Ways According to Stimulus Dose
- 3-2. The Identity of Acupuncture — Mechanical Signals Sent to Connective Tissue and Dose-Response
- 3-3. External Treatment ① Mechanical Axis — Two Axes: Stimulus Intensity and Mode of Action
- 3-4. External Treatment ② Thermal Axis — Heat-Assisted Moxibustion (Sustained Deep Heat Transfer)
- 3-5. External Treatment ③ Pharmacological Axis — Bee Venom Acupuncture and Herbal Acupuncture (Inflammation Control and Local Cleansing and Regeneration)
- 3-6. Internal Treatment (內治) — Managing Left-Side Biochemical Environment with Herbal Medicine
- 3-7. Integration — Six-Stage Coordinates of Three External Treatment Axes and Internal Treatment
- 4. Cross-Reading (Discussion)
- 5. What Remains Unknown (Limitations)
- 6. References
Connective Tissue Adaptive Response According to Stimulus Dose and an Integrated Model of Korean Medicine External and Internal Treatment — A Literature Review on the Action Coordinates of Acupuncture, Acupotomy, Heat-Assisted Moxibustion, Bee Venom Acupuncture, and Herbal Medicine
1. Key Summary (Abstract)
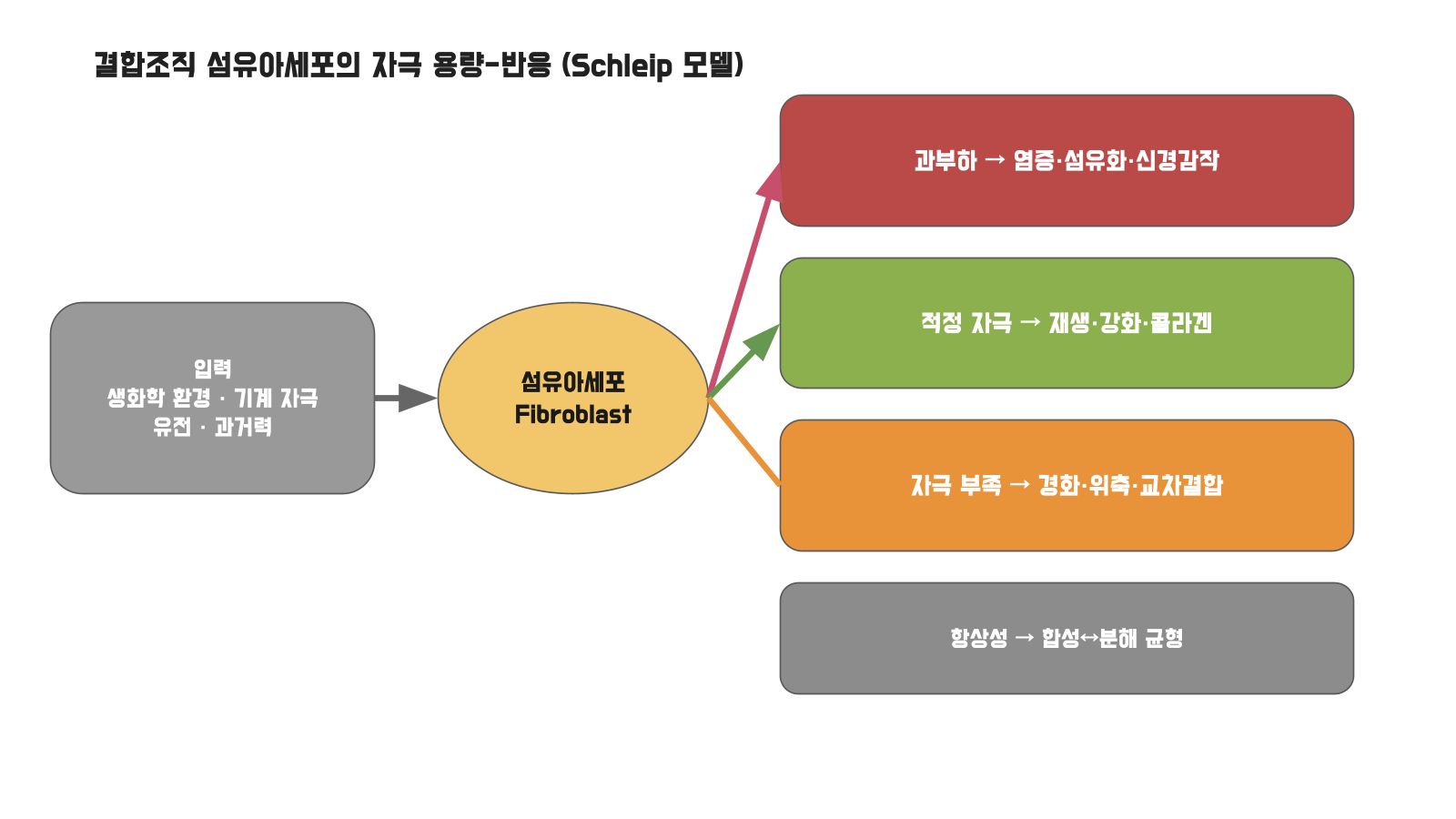
The recurrence of chronic pain even after treatment is commonly interpreted as "treatment was ineffective." However, from the perspective of connective tissue mechanobiology, this occurs because the mechanical and biochemical environment of the tissue that created the pain remains unchanged. Fibroblasts in connective tissue respond in three distinct ways depending on stimulus dose — excess causes inflammation, fibrosis, and central sensitization; deficiency causes stiffening, atrophy, and cross-linking; optimal dosage produces collagen regeneration and strengthening. The essence of treatment is not to eliminate stimulus, but to move trapped tissue into the optimal range. This paper divides external treatment into three axes — ①mechanical axis that directly handles tissue (acupuncture, acupotomy, thread embedding), ②thermal axis that delivers heat to deep tissue (heat-assisted moxibustion), ③pharmacological axis involved in inflammation, cleansing, and regeneration (bee venom acupuncture, herbal acupuncture). On the mechanical axis, we must distinguish the "intensity" of stimulus (rotation, depth, gauge) from the "mode of action" of needle tip (conical compression versus blade-like cutting), which explains the role division between acupuncture and acupotomy. If external treatment addresses local input on the right, internal treatment (herbal medicine, constitutional detoxification) manages the whole-body biochemical milieu on the left side of the diagram. The six-stage roadmap places this stepwise on the dose-response curve. However, direct clinical evidence for later stages (detoxification, constitutional conditioning) and thread embedding is weak, and this paper presents them as a hypothetical integrated model.
2. Context of the Question (Introduction)
"The pain was better after injections and acupuncture, but a few days later, the same area hurts again." Clinicians tend to interpret this repetition as "insufficient intensity" or "an inherently incurable disease," but both interpretations view pain as a singular event. The past two decades of connective tissue mechanobiology have challenged this notion. Fibroblasts in tendons, ligaments, and fascia are active cells that sense mechanical environment and remodel the extracellular matrix (ECM), a process called mechanotransduction. Khan and Scott brought this into clinical practice and revived "mechanotherapy" (Khan & Scott, 2009). The crucial fact is that the same load produces opposite results depending on dose — deficiency causes stress-shielding, excess causes fibrosis, and there is an optimal range between them that maximizes regeneration. Korean medicine has approached this curve with two hands: external and internal treatment.
3. What the Literature Says (Results)
3-1. Connective Tissue Responds in Three Ways According to Stimulus Dose
Mechanical stimulus induces TGF-β1 and type I collagen expression in fibroblasts (PMC4509256). However, this is not a simple linear increase. In three-dimensional models, as deformation amplitude increased, proliferation occurred simultaneously with myofibroblast transition (fibrosis), and approximately 2.5-fold proliferation was observed at 12% deformation (Sci Rep, 2022). Loss of load results in loss of strength and alignment (stress-shielding). M1 macrophage phenotype switches at even 3% deformation (Babaniamansour et al., 2023). Ligament fibroblasts have optimal deformation parameters (PMC4976179). This three-way model was formalized by Schleip, based on the principle that fibroblasts adapt connective tissue morphology to repeated loading (Schleip & Müller, 2013; Schleip & Baker, 『Fascia in Sport and Movement』). Homeostatic matrix remodeling in the optimal range is explained by the fact that tissue remodeling depends on mechanical environment history and genetics, with use promoting and disuse delaying the process (Cowin, 2004).
3-2. The Identity of Acupuncture — Mechanical Signals Sent to Connective Tissue and Dose-Response
Langevin et al. proposed that "arrival of qi" and "needle grasp" originate from needle-connective tissue mechanical coupling and transmit mechanical signals to cells (Langevin et al., 2001). When needles are rotated, subcutaneous fibroblasts reorganize their scaffold, with response peaking at 2 rotations and declining beyond that (Langevin et al., 2006). Acupuncture is a dose-adjustment device for mechanical stimulus; excessive stimulation reduces response.
3-3. External Treatment ① Mechanical Axis — Two Axes: Stimulus Intensity and Mode of Action
The mechanical axis divides into two axes: one is stimulus intensity (how strongly the same action is applied), the other is mode of action (what type of work is done).
(a) Stimulus Intensity Axis — Dose Variations in Acupuncture. Round conical filiform needles compress and penetrate tissue to stimulate it. Intensity is controlled by rotation frequency (Langevin's two-rotation peak), depth, gauge, and force. The effect of depth is confirmed clinically — in shoulder fascia pain syndrome, deep needling was superior to shallow 2mm needling at termination, 1-month, and 3-month follow-up (Ceccherelli et al., 2001). Intensity has the same effect, with high-intensity electroacupuncture significantly raising pain pressure threshold compared to placebo (Barlas et al., 2006). Increased intensity with needle gauge has not been directly verified by RCT, but it is mechanically evident that thicker gauges increase tissue deformation and needle grasp area.
(b) Mode of Action Axis — Differentiation Between Filiform and Blade Needles. No matter how much intensity is increased, filiform needles cannot cut fibers with their round tips; they only push tissue. Acupotomy uses blade-shaped needle tips to cut and separate adhesive fascia and ligaments. This is not a matter of intensity but a separate procedure with a different mode of action. Severely stiffened adhesions are in the deficiency range where stress-shielding prevents stimulus from reaching them, and cannot be separated even with thick, strong filiform needles — a tangled knot cannot be loosened by driving in a thick nail forcefully; it must be cut. Light adhesions may be separated by thick filiform needles, but stiffened adhesions require acupotomy. Acupotomy is a procedure that opens an entry path to tissue unreachable by stimulus, and only when that path is opened does the ensuing stimulus (②–③) work.
(c) Thread Embedding — Duration Axis. Thread embedding uses absorbable thread to leave low-intensity sustained stimulus lasting days to weeks. Evidence level is low, with thread embedding at acupoints for chronic low back pain remaining at the protocol stage (Zhong et al., 2022).
In summary, filiform needles control intensity, acupotomy controls mode of action, and thread embedding controls duration.
3-4. External Treatment ② Thermal Axis — Heat-Assisted Moxibustion (Sustained Deep Heat Transfer)
This paper addresses heat-assisted moxibustion where, after needle insertion, the needle handle is heated to deliver heat through the needle shaft to deep ligaments and fascia in a sustained manner. Rather than burning the surface, it minimizes skin damage while delivering heat deeply. The efficacy of warm needling techniques is supported by meta-analysis, showing superiority in efficacy rate, pain reduction, and functional improvement in knee osteoarthritis compared to other traditional treatments (Jin & Guan, 2022). Heat-assisted moxibustion is a procedure targeting the optimal range (soft tissue strengthening) by continuously delivering appropriate thermal stimulus to deep tissue to induce blood flow and collagen regeneration.
3-5. External Treatment ③ Pharmacological Axis — Bee Venom Acupuncture and Herbal Acupuncture (Inflammation Control and Local Cleansing and Regeneration)
The third axis is the action of injected substances. Bee venom acupuncture and herbal acupuncture operate differently, and herbal acupuncture has many branches within itself.
Bee Venom Acupuncture (蜂鍼) operates through chemical, immune, and neural pathways. NF-κB inhibition by melittin, the main component of bee venom, is identified as the key mechanism of anti-inflammatory and anti-arthritic effects (Son et al., 2007; Bhardwaj et al., 2025), while analgesia from bee venom acupuncture is explained through central mechanisms including spinal opioid, α2-adrenergic, descending serotonin, and c-Fos inhibition (Son et al., 2007). Bee venom acupuncture pulls the overload range (inflammation, central sensitization) down through chemical, immune, and neural pathways.
Herbal Acupuncture (藥鍼) is not a single treatment. The spectrum of action is broad depending on injected herbal materials, formulation, and concentration, making it difficult to reduce to a single mechanism. Expected actions generally move in three directions, with emphasis varying by herbal acupuncture type. First, physical effects (volume and cleansing) — the volume of injectate separates adhesive soft tissue and dilutes and expels local inflammatory products, which appears to be an effect shared by injection procedures generally rather than a mechanism unique to Korean medicine herbal acupuncture (for reference, literature reviews of ultrasound-guided hydrodissection in Western medicine note that injectate mechanically separates and decompresses trapped nerves and soft tissue — Buntragulpoontawee et al., 2021). Second, anti-inflammatory and pharmacological actions are proposed for herbal acupuncture (with bee venom acupuncture as exemplary). Third, approaches targeting tissue regeneration — when actively anticipating collagen regeneration and strengthening, evidence is relatively more abundant in placental extract (porcine placenta) and salmon DNA (PDRN) categories. Placental extract acupuncture is being reviewed in chronic musculoskeletal pain (Kim et al., 2020), and PDRN — while being research on injectable medication rather than Korean medicine herbal acupuncture — has reported collagen synthesis and tensile strength recovery in animal tendon injury (Kang et al., 2018) and improved tendon healing and reduced fatty degeneration in rotator cuff repair (Hwang et al., 2021). This is a reference for "what categories could be considered if regeneration is the goal," not a claim that all herbal acupunctures have regenerative effects. In summary, it is inaccurate to lump herbal acupuncture as "pharmacologically regenerating" or to dismiss it as "merely cleansing"; herbal acupuncture is a broad spectrum with varying proportions of physical, anti-inflammatory, and regenerative effects depending on type, operating in the diagram from the overload range (cleansing and anti-inflammation) to the optimal range (regeneration).
3-6. Internal Treatment (內治) — Managing Left-Side Biochemical Environment with Herbal Medicine
On the left side of the diagram is another input — biochemical environment, genetics, and history. The same stimulus becomes overload if the environment is poor. Obesity is a state of chronic low-grade inflammation where adipokines contribute to tendon disease, and weight loss improves symptoms (Castro et al., 2016). Obesity, metabolic syndrome, and musculoskeletal disease share common NFκB and MAPK inflammatory pathways (Collins et al., 2018). Pain is a function of central sensitization, not injury magnitude, and central sensitization depends on systemic inflammatory environment (Dean et al., 2013). Korean medicine internal treatment targets this environment. Narrowly, Peony and Licorice Decoction alleviates muscle cramps and tension (Ai et al., 2006; Mitsumoto et al., 2023), and formulas like Eucommia and Rehmannia Pills are reviewed in clinical research for low back pain and radicular pain (Goo et al., 2018; Sung et al., 2019). Broadly, constitutional detoxification and fasting detoxification "cleanse" (empty) systemic inflammation and metabolic burden, and constitutional-customized prescriptions "fill" (condition) the regeneration foundation on top. Cleansing comes first, filling comes later.
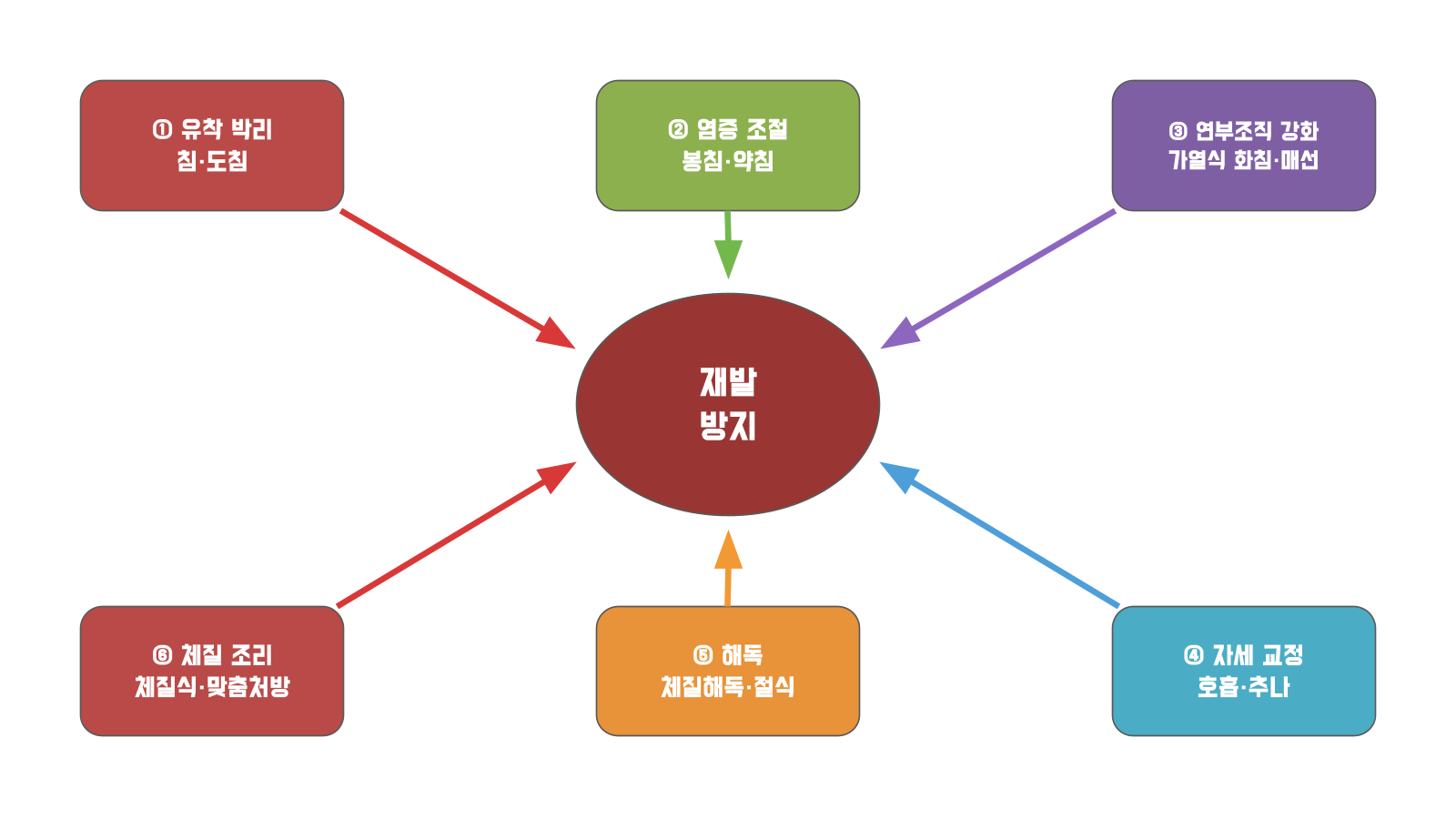
3-7. Integration — Six-Stage Coordinates of Three External Treatment Axes and Internal Treatment
①–③ are local external treatment, ④ is loading pattern, ⑤⑥ are internal treatment. Pain that "returns even after treatment" occurs when ①–③ stop short, touching only the local area while neglecting ⑤⑥ (systemic environment).
4. Cross-Reading (Discussion)
| Category | Range of Operation | Pathway |
|---|---|---|
| External Treatment-Mechanical (Intensity) | Local, Immediate | Stimulus Variation (rotation, depth, gauge) |
| External Treatment-Mechanical (Mode of Action) | Local, Immediate | Cutting and Separation (acupotomy) |
| External Treatment-Thermal | Local, Deep | Sustained Deep Heat Transfer (heat-assisted moxibustion) |
| External Treatment-Pharmacological | Local-Systemic Border | Cleansing, Anti-inflammation, Regeneration (bee venom acupuncture, herbal acupuncture) |
| Internal Treatment | Systemic, Foundational | Metabolic and Inflammatory Environment Adjustment (herbal medicine, detoxification, constitutional conditioning) |
External treatment moves one point on the curve by hand, while internal treatment tilts the coordinate plane on which the curve is drawn. Bee venom acupuncture is external treatment with chemical and neural pathways, standing at the boundary between both. Eliminating pathogenic factors corresponds to overload and cleansing the left-side environment, while supporting righteous qi corresponds to filling the regeneration foundation. Answer to "wouldn't thick filiform needles make acupotomy unnecessary?" — intensity and mode of action are different dimensions; cutting severe adhesions cannot be substituted by increased stimulus. In evidence hierarchy, ①③④ and ② (especially bee venom acupuncture) are relatively robust, while ⑤⑥ and thread embedding have weak direct evidence compared to mechanistic coherence, so they are distinguished as hypothetical extensions.
5. What Remains Unknown (Limitations)
- The diagram is specified by the Schleip model, but Korean medicine application interpretation requires additional validation.
- Due to access restrictions on mediclassics.kr, direct comparison of original Chinese texts for 痺論 (Bi Lun) and 經筋 (Jing Jin) was impossible, so citations were made only at the title and chapter level.
- Depth (Ceccherelli) and intensity (Barlas) have evidence, but no sole-gauge RCT exists, so it was described as evident inference.
- Quantitative criteria for the boundary between filiform and blade needles are absent, depending on clinical judgment.
- Herbal acupuncture has highly variable formulations and materials, so the three-way classification of physical, anti-inflammatory, and regenerative effects in this paper is illustrative of the action spectrum rather than comprehensive, and cited PDRN and hydrodissection are Western medicine injectable studies rather than Korean medicine herbal acupuncture, referenced only as analogy.
- Direct RCTs of ⑤⑥'s pain effects are unconfirmed; indirect inference through systemic inflammation and metabolic mechanisms.
- No method exists to convert cell model deformation amplitude (3, 6, 12%) to needle stimulus dose.
6. References
Khan KM, Scott A. 2009. Br J Sports Med 43(4):247-252. https://doi.org/10.1136/bjsm.2008.054239
Sci Rep 2022. https://doi.org/10.1038/s41598-022-20383-5
Babaniamansour P, et al. 2023. Tissue Eng Part A 30(7-8):314-329. https://doi.org/10.1089/ten.TEA.2023.0110
PMC4976179 (ligament optimal deformation parameters)
PMC4509256 (mechanical stimulus → TGF-β1, type I collagen)
Dean BJF, et al. 2013. Clin Orthop Relat Res 471(9):3036-3046. https://doi.org/10.1007/s11999-013-3010-y
Langevin HM, et al. 2001. FASEB J 15(12):2275-2282. https://doi.org/10.1096/fj.01-0015hyp
Langevin HM, et al. 2006. J Cell Physiol 207(3):767-774. https://doi.org/10.1002/jcp.20623
Ceccherelli F, et al. 2001. Acupunct Electrother Res 26(4):229-238. https://doi.org/10.3727/036012901816355938
Barlas P, et al. 2006. Pain 122(1-2):81-89. https://doi.org/10.1016/j.pain.2006.01.012
Chen H, et al. 2024. Curr Pain Headache Rep 28(7):709-722. https://doi.org/10.1007/s11916-024-01242-6
Liu CY, et al. 2024. BMJ Evid Based Med 29(6):374-384. https://doi.org/10.1136/bmjebm-2023-112626
Jin S, Guan X. 2022. Ann Palliat Med 11(2):708-716. https://doi.org/10.21037/apm-21-3972
Zhong G, et al. 2022. Medicine 101(52):e32409. https://doi.org/10.1097/MD.0000000000032409
Son DJ, et al. 2007. Pharmacol Ther 115(2):246-270. https://doi.org/10.1016/j.pharmthera.2007.04.004
Bhardwaj V, et al. 2025. Naunyn Schmiedebergs Arch Pharmacol 398(8):9797-9815. https://doi.org/10.1007/s00210-025-03991-6
Goo B, et al. 2018. Medicine 97(50):e13684. https://doi.org/10.1097/MD.0000000000013684
Sung WS, et al. 2019. Trials 20(1):778. https://doi.org/10.1186/s13063-019-3776-7
Ai M, et al. 2006. World J Gastroenterol 12(5):760-764. https://doi.org/10.3748/wjg.v12.i5.760
Mitsumoto H, et al. 2023. Trials 24(1):449. https://doi.org/10.1186/s13063-023-07424-8
Castro AAE, et al. 2016. Arq Bras Cir Dig 29(Suppl 1):107-110. https://doi.org/10.1590/0102-6720201600S10026
Collins KH, et al. 2018. Front Physiol 9:112. https://doi.org/10.3389/fphys.2018.00112
『Yellow Emperor's Classic of Internal Medicine (Huangdi Neijing)·Simple Questions (Suwen)』 Bi Lun (Impediment Discussion) / 『Spiritual Axis (Lingshu)』 Jing Jin (Meridian Sinews) / 『Exemplary Cases of the Eastern Medical Treasure Compendium (Dongyi Baojian)』 External Forms Section, Sinew (titles and chapter levels only)
Schleip R, Müller DG. 2013. J Bodyw Mov Ther 17(1):103-115. https://doi.org/10.1016/j.jbmt.2012.06.007 (+ Schleip & Baker, 『Fascia in Sport and Movement』 — primary source of diagram)
Cowin SC. 2004. Annu Rev Biomed Eng 6:77-107. https://doi.org/10.1146/annurev.bioeng.6.040803.140250
Buntragulpoontawee M, et al. 2021. Front Pharmacol 11:621150. https://doi.org/10.3389/fphar.2020.621150
Kim J, et al. 2020. Trials 21(1):525. https://doi.org/10.1186/s13063-020-04442-8
Kang SH, et al. 2018. J Orthop Res 36(6):1767-1776. https://doi.org/10.1002/jor.23796
Hwang JT, et al. 2021. Tissue Eng Regen Med 18(6):1009-1020. https://doi.org/10.1007/s13770-021-00378-5
Choi Jang-Hyeok | Korean Medicine Practitioner, Director of Dongjedang Korean Medicine Clinic | Research Method: DJD Multi-Literature Cross Research
Connective TissueMechanobiologyPain ManagementExternal and Internal TreatmentFibroblastDose-ResponseKorean Medicine ResearchIntegrative Medicine